Ryan A. Anderson, D.O.
Chief Resident, Lehigh Valley Health Network
CASE
A 33-year-old male is brought to the emergency department after being found down in his bathroom. He is slightly confused but has normal vital signs. A white powder was found at the scene, and the patient claims he was snorting crushed up Wellbutrin pills.
DISCUSSION
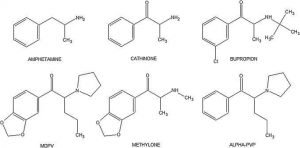
Physicians are prescribing bupropion for several different indications, and it is becoming more ubiquitous in the community. It is marketed as an antidepressant (Wellbutrin®), smoking cessation aid (Zyban®), and dieting agent (Contrave®). It is also quickly becoming a popular drug of abuse. Some users describe the high as similar to cocaine or methamphetamine but with less intensity. This isn’t surprising given the chemical structure of bupropion closely resembles that of methamphetamine. Bupropion is the only synthetic cathinone (a class of drugs commonly known as “bath salts”) approved by the FDA. (Figure 1). Its mechanism of action is achieved through inhibition of norepinephrine and dopamine reuptake, and antagonism at nicotinic receptors. Due to its relatively low cost and ease with which it may be obtained, bupropion has been named the “poor man’s cocaine.”
The hallmark of bupropion toxicity is seizures. Seizures occur in a dose-dependent fashion and are even seen at therapeutic drug concentrations. Some poison databases have shown bupropion to currently be the most common cause of medication-induced seizures. Wellbutrin® comes in immediate-release (IR), sustained release (SR), and extended-release (XR). Both SR and XR formulations may cause delayed seizures and most patients require 24 observation period following an intentional ingestion.
Insufflation or “snorting” bupropion is a recently described phenomenon although it has already been seen within the Lehigh Valley community in Pennsylvania. Reported effects may include euphoria, tachycardia, agitation, hallucinations, and seizures. The nasopharynx contains a highly vascularized surface area that allows for drugs to readily enter systemic circulation. It is a common route of administration for other commonly abused drugs such as cocaine, heroin, and methamphetamine.
Lewis JC et al performed an observational study in 2014 describing 67 cases of isolated bupropion insufflation over an 11-year period using the California Poison Control System. The mean dose was 1500mg. The most common finding was tachycardia, with agitation and tremors also being commonly observed. 30% of the patients in this study sustained prehospital seizures. Seizures typically occurred within 8 hours which is more rapid than the delayed seizures reported following oral ingestions. The crushing of pills destroys the properties that enable a pill to be sustained-release or extended-release. Bupropion overdoses may cause significant cardiotoxicity as well although this hasn’t been yet reported with insufflation. All patients with bupropion exposures should have an EKG obtained.
Figure 1
Case Conclusion:
The patient’s partner arrives and is able to confirm that the patient experienced a tonic-clonic seizure approximately 15 minutes after bupropion insufflation. His mental status returns to baseline and he has a normal glucose, EKG, vital signs, and neurological examination. He is observed in the ED for 8 hours and then discharged home with resources for drug counseling.
RESOURCES
British Columbia Drug and Poison Information Centre (BC DPIC), www.dpic.org/article/professional/focus-bupropion-toxicity-and-abuse.
Kriikku P, Ojanperä I. The relationship between bupropion and suicide in post-mortem investigations. Forensic Sci Int. 2016;266:343-348.
Hill S, Sikand H, Lee J. A case report of seizure induced by bupropion nasal insufflation. Prim Care Companion J Clin Psychiatry. 2007;9(1):67-9.
Welsh CJ, Doyon S. Seizure induced by insufflation of bupropion. N Engl J Med. 2002;347(12):951.
Thundiyil JG, Kearney TE, Olson KR. Evolving epidemiology of drug-induced seizures reported to a Poison Control Center System. J Med Toxicol. 2007;3(1):15-9.
Lewis JC, Sutter ME, Albertson TE, Owen KP, Ford JB. An 11-year review of bupropion insufflation exposures in adults reported to the California Poison Control System. Clin Toxicol (Phila). 2014;52(9):969-72.